
 The practice of Hadi Zambarakji
The practice of Hadi Zambarakji
Newsletter Summer 2014
Issue 3.1
Dear patients and friends,
I suppose I do not have much of an excuse for not updating the newsletters as often as I should, even though I really enjoy writing the newsletter. Clinically, I have been busy both in the NHS and in my private practice. At Whipps Cross Hospital, we are now well into the partnership with Barts NHS Trust and Newham NHS Trust to form the largest organization in the UK; this is Barts Health of course. The immediate impact on my NHS practice was an increase in the number of referrals with Vitreoretinal diseases, which I was very pleased about. I have been fortunate to have a very dedicated new training Vitreoretinal Fellow who is most reliable, so a definite budding Vitreoretinal Surgeon. I have also been busy pursuing my research interests and I am glad to say that we have had several accepted publications, spanning diabetic retinopathy, myopic eye disease and macular hole surgery and choroidal imaging. Finally I have pursued my interests as an examiner for the Royal College of Ophthalmologists, something I started 3 years ago and I enjoy thoroughly. At home, it is been a pleasure watching our new arrival Raphael develops amongst his brothers Adam 9 and Daniel 6. As always I would welcome your ideas for topics for the next newsletter.

Hadi Zambarakji MB ChB, FRCOphth, D.M
info@retinacare.org.uk
Spire Roding Hospital, Roding Lane South, Ilford. IG4 5PZ.
Gadgets in Ophthalmology…
Ophthalmologists generally love new tools and I am very keen on novel technology. So we have moved from having a retinal camera (which we still need of course) to having Optical Coherence Tomography (OCT) scans, which can image the retina live with a fantastic amount of detail. For the management of patients with retinal disease, we used to rely on fundus fluorescein angiography (FFA), a test which involved the injection of a fluorescent dye into one of the veins of the forearm. Whilst we still need FFA, we would now monitor for further change using OCT, so no need for more injections. OCT scans take 3-5 minutes, do not involve an injection and give plenty of information, which sometimes cannot be seen clinically. OCT scans because available about 10-12 years ago, but today form part of any retinal practice. What is most impressive, is that OCT imaging not only allows the Ophthalmologist to image the retina, but it is also possible to image the layers behind the retina called the choroid, as well as the optic nerve. Their use has therefore spread to the glaucoma specialist as well as the neurologist. New OCT scanners are so developed, that some can combine OCT and fluorescein angiography, and the very newest machines can perform OCT/angiography without the injection of a fluorescent dye! The new OCT/angiography instruments are only just being marketed, so not available widely just yet.
For those with retinal disease and especially macular diseases such as macular hole, epiretinal membrane, diabetic retinopathy and macular degeneration, an OCT scan today would be a routine standard investigation. OCT not only image the retina at presentation, but allow the clinician to monitor progress and response to treatment. In the case of a macular hole, it may show closure of the hole after surgery (figure 1), but in the case of diabetic retinopathy, it would show improvement (or not) of the macular thickness and macular oedema after treatment with laser or intravitreal injections (figure 2). Most patients in my clinic would therefore have the vision check, followed by eye drops to dilate the pupil then a OCT scan before seeing me.
Figure 1a: OCT scan shows a macular hole with markedly reduced vision in a 55 year-old patient right eye
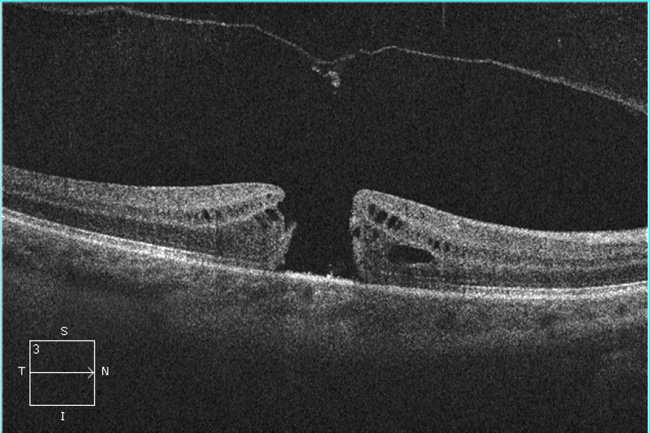
Figure 1b: OCT scan of the retina 6 weeks after vitrectomy surgery (same eye as in figure 1a): the macular hole is closed and the vision has improved already by 2 lines.
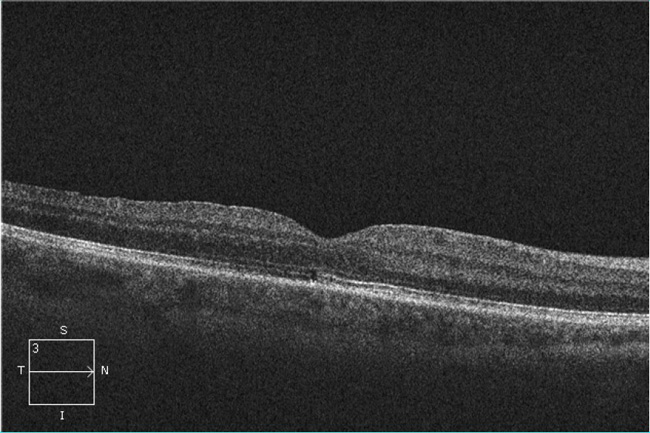
Figure 2a: The OCT scan on the left in a 57 year-old patient with reduced vision due to diabetic macular oedema shows a large cyst in the retina. The OCT scan on the right (3 months after treatment intravitreal Lucentis) shows total resolution of the cyst and improved vision.
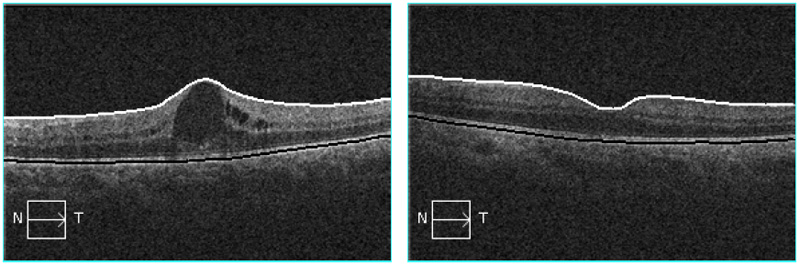
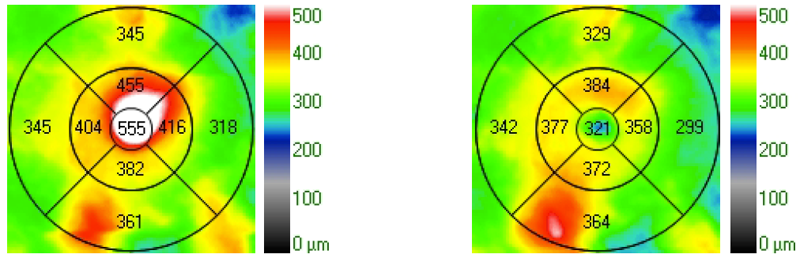
Figure 2b: The macular thickness map on the left (before treatment) shows a markedly increased thickness of the retina (555 microns) and on the right (3 months after treatment with intravitreal Lucentis) the macular thickness has gone back to almost normal (321 microns)
Along with the new developments, are software developments, which allow a clinician to view all tests on one computer station, without the need to run around between machines to view results? More impressive, is that software developments with networking capabilities allow the integration of imaging done in clinic with equipment elsewhere such as the operating room and operating microscope. In the setting of cataract surgery for instance, and in particular if planning to implant a toric intraocular lens implant to correct for astigmatism as well as well remove the lens opacity (the cataract), the measurements for the lens are done in clinic using a biometry instrument. The newer biometry instruments take a picture of the eye at the same time. The exact axis of alignment for the toric lens implant is determined after measuring the degree of corneal astigmatism. This information is relayed via appropriate software to the operating microscope via the hospital network. The surgical plan uses the image of the eye, to identify the 0-180 reference plane and maps on the microscope image the axis of alignment for the toric lens implant. This not only helps more accurate placement (to correct astigmatism) of a toric lens implant, but also removes the need to mark the eye pre-operatively (which we would normally do to identify the 0-180 reference plane).
I can’t hide the fact of course that hospital managers do not like it when I go to their offices, as I am constantly after funding for more equipment, software or as they call it “expensive gadgets” … but this is what makes Ophthalmology so special.
In my next newsletter, I will discuss my involvement with a program for phaco cataract surgery and implantation of an intraocular telescope (this is different form the standard intraocular implant) in patients with advanced age-related macular degeneration. This is a new development, which will probably make a significant difference to at least some patients who have this difficult condition.
Hadi Zambarakji
No comments yet
Leave a comment
Search the RetinaCare website
Newsletter Archive
![]() Retinacare Newsletter Issue 8.2 (November 2025)
Retinacare Newsletter Issue 8.2 (November 2025)
![]() Retinacare Newsletter Issue 8.1 (January 2025)
Retinacare Newsletter Issue 8.1 (January 2025)
![]() Retinacare Newsletter Issue 7.1 (January 2021)
Retinacare Newsletter Issue 7.1 (January 2021)
![]() Retinacare Newsletter Issue 6.2 (December 2018)
Retinacare Newsletter Issue 6.2 (December 2018)
![]() Retinacare Newsletter Issue 6.1 (November 2018)
Retinacare Newsletter Issue 6.1 (November 2018)
![]() Retinacare Newsletter Issue 5.1 (Spring 2016)
Retinacare Newsletter Issue 5.1 (Spring 2016)
![]() Retinacare Newsletter Issue 4.1 (Spring 2015)
Retinacare Newsletter Issue 4.1 (Spring 2015)
![]() Retinacare Newsletter Issue 3.1 (Summer 2014)
Retinacare Newsletter Issue 3.1 (Summer 2014)
![]() Retinacare Newsletter Issue 2.1 (Summer 2013)
Retinacare Newsletter Issue 2.1 (Summer 2013)
![]() Retinacare Newsletter Issue 1.3 (Winter 2012)
Retinacare Newsletter Issue 1.3 (Winter 2012)
If you are subscribed and don’t wish to receive any further newsletters, please email: info@retinacare.org.uk
News & GP Articles
 Management of advanced diabetic eye disease:
Management of advanced diabetic eye disease:
Diabetic Eye Journal; March 2014
Delivering drugs to the retina:
Newsletter for GPs Holly House Hospital; Winter 2014 (page 8)
Diabetic macular oedema:
Practice matters issue 14; December 2013
Guide to Vitrectomy for Floaters
Guide to 23 gauge vitrectomy surgery
Useful links
Certificate of Vision Impairment (CVI) Registration:
The Royal College of Ophthalmologists:
This should probably the first site accessed by anyone in the UK who would like to obtain information about eye care. The College provides valuable support for professionals and patients.
The National Institute for Health and Care Excellence (NICE):
NICE Supports healthcare professionals and others to make sure that the care they provide is of the best possible quality. NICE provide independent, authoritative and evidence-based guidance on the most effective ways to prevent, diagnose and treat disease and ill health, reducing inequalities and variation.
BEAVRS:
BEAVRS is the acronym for the British and Eire Association of Vitreoretinal Surgeons. The aim of the Association is to promote high quality patient care by supporting and representing British and Irish Vitreo-Retinal Surgeons through education, research, audit and revalidation.
Euretina:
This should probably the first site accessed by anyone in the UK who would like to obtain information about eye care. The College provides valuable support for professionals and patients.
The Macular Society:
This society has been supporting people with macular conditions, including age-related macular degeneration (AMD), for 25 years. The society offers information and support while funding research to find a cure. All services are free so that no one has to face a macular condition alone. This is the best site in the UK if you are a patient with macular degeneration and would like to know more and seek where can you get support.
Royal National Institute of Blind People (RNIB):
The RNIB is the leading charity offering information, support and advice to almost two million people with sight loss. The RNIB provide practical ways to help patients live with sight loss, and give advice to help travel, shop and manage money and finances independently. The RNIB also give advice on technology for blind and partially sighted people.
The British Medical Association (BMA):
The BMA stand up for doctors both individually and collectively on a wide variety of employment issues and, since the inception of the NHS, have been formally recognised for collective bargaining purposes within national negotiating machinery and by individual employers at local level.
The “access to work program”:
This government program helps pay for practical support so anyone with a disability can do their job (in the case of my patient, this is usually a visual disability). This is free of charge to anyone in the UK.
www.gov.uk/access-to-work/overview
The implantable intraocular telescope for patients with advanced age-related macular degeneration:
The CentraSight treatment programme uses a tiny telescope, which is implanted inside the eye to improve vision and quality of life for individuals affected by end-stage age-related macular degeneration. The above link allows the patient to find the necessary information about this program. Mr. Hadi Zambarakji is currently in the process of developing a patient pathway and will be offering with CentraSight this new technology to his patients.