
 The practice of Hadi Zambarakji
The practice of Hadi Zambarakji
Guide to Macular holes
THE RETINA
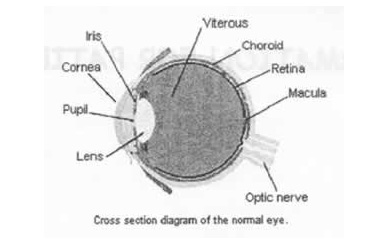
The retina is the light sensitive layer at the back of the eye (film), which transmits the messages along the optic nerve to the brain. Light rays enter the eye through the transparent (clear) cornea, and must pass through the lens and vitreous (a jelly-like substance) before reaching the retina.
Unlike a camera, the image obtained by the retina is not of uniform clarity or sharpness. Only the central portion of the retina, the macula, is sensitive enough to provide high quality vision for tasks such as reading, watching television, or driving. The macula is the central part of the retina, which is capable of the detailed vision, necessary for tasks such as reading.
FORMATION OF A MACULAR HOLE
The central portion of the eye is filled with a jelly-like substance known as the vitreous. As a person ages, the vitreous ‘jelly’ begins to shrink, being replaced by fluid. As the vitreous shrinks, it pulls away from the surface of the retina. In most cases, this pulling away or vitreous separation occurs without any negative effect. In a small number of cases, shrinkage and movement of the vitreous can result in the formation of a hole in the macular region, known as a macular hole. This process results in a defect or dark spot in the central vision with distortion and in the longer term severe loss of central vision.
SYMPTOMS
Decreased central vision for both distance and reading activities, distortion in central vision and a defect in the central vision where letters may disappear.
TREATMENT
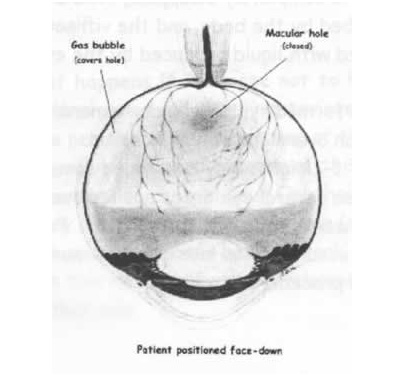
It is possible to offer a surgical procedure with the potential for some visual improvement. This procedure is known as a Vitrectomy, and involves the removal of the vitreous jelly within the centre of the eye. A large gas bubble is placed within the vitreous cavity of the eye, which, when it comes into contact with the retina, presses it against the wall of the eye, sealing the macular hole. This process acts much like a hand holding wallpaper against the wall permitting it to stick and remain in position as the ‘wallpaper glue’ dries. The procedure includes peeling of a thin membrane around the macula hole called the inner limiting membrane, which helps improve the closure rate of the macular hole.
In order to be effective, the bubble must apply continued upward pressure against the retinal surface in the area of the macula. There have been several changes during the last 2-4 years in macular hole surgery. Some of these advances relate to the use of small gauge instruments through small key holes which usually but not always do not require surturing, thus providing more comfort after surgery (see 23 gauge vitrectomy handout). I currently routinely use small gauge instruments for macular hole surgery (23 gauge vitrectomy) and almost always would perform surgery under local anaesthesia.
Other advances relate to the use of a shorter acting gas bubble because we now know that most of the closure of the macular hole occurs during the first week post operatively. Therefore if the hole does not close early, it will probably not be closed when the patient is examined 3-4 weeks later after the gas has reabsorbed. It therefore does not make sense to use a long acting buble of gas unless there are other reasons for doing so.
The last comment of interest is around the need for post-operative posturing. We used to advise patients to remain in a ‘face down’ position to allow the bubble to rise toward the back of the eye and exert pressure to close the hole. We know have reasonably good evidence to demonstrate that posturing for 3-5 days is probably sufficient in the majority of patients and for some patients, no posturing at all may be necessary.
My recommendations have therefore changed to the following:
I would recommend that patients with small macular holes of a recent onset do not need to posture at all (except that I ask the patient NOT to lie on their back), and for those with larger macular holes and in particular for patients with longer standing holes (ie more than 4 months), I would recommend 5 days of face down positioning for 45 minutes every hour.
The gas bubble may take anywhere from 2-4 weeks following surgery to completely disappear. The bubble is gradually reabsorbed by the body, and the vitreous cavity is then filled with liquid produced by the eye.
The surgery is performed typically under local anaesthesia, and sometimes combined with phaco cataract surgery. You will need to use 3 or 3 types of eye drops applied over the 4 weeks following the surgery. Full visual recovery may not occur until as late as three months after the surgical procedure.
GENERAL QUESTIONS
Q: Is a macular hole the same as macular degeneration?
A: No, macular holes and macular degeneration are two distinct conditions. Macular degeneration refers to wear and tear of the central retina, and in some occasions is associated with severe vision loss due to leakage and haemorrhage in the central retina. For details please see information handout on macular degeneration. A macular hole involves the formation of a hole on the inner side of the retinal surface, as a result of traction at the junction between the vitreous and the retina.
Q: If I have a macular hole in one eye, does this mean I could get the same in the other eye?
A: There is on average, a 5-10% a risk of developing a macular hole in the other eye, this risk depends on the state of the “vitreous jelly”.
Q: Does it matter how long I have had the macular hole if I am interested in having surgery done?
A: Macular holes present for less than six months have a better chance of repair and visual recovery than those present for more than six months. Optimal visual outcomes are obtained if surgery is performed within the first 2 months of the development of symptoms. Surgery is not usually recommended for macular holes which have been present for more than one year as the success rate is low.
Q: When will I get my vision back?
A: While the gas bubble is present in the eye, vision is very blurred. As the bubble begins to shrink, vision begins to return. Final vision recovery is often not achieved for 3-4 months following the operation. If you have not had cataract surgery, the vision may begin to exhibit gradual deterioration approximately 6-12 months after the operation as a cataract develops. I would almost always recommend to perform phaco cataract surgery at the same time of macular hole surgery in patients over the age of 50 years in order to avoid a second procedure for removal of the cataract.
Q: Am I able to travel after macular hole surgery?
A: You should not travel by air if you have had gas injected and the bubble is still present – this period can last up to 6 weeks if a long acting gas has been used. The depressurisation will cause the gas bubble to expand and your eye to become very painful. Please check with your Ophthalmologist before you travel by air. The gas buble would also expand if you go up to high altitude, the same recommendations would therefore apply.
THE SAME APPLIES IF YOU HAVE AN EMERGENCY AND NEED TO HAVE AN URGENT ANESTHETIC WHILST THE GAS BUBBLE HAS NOT FULLY REABSORBED, PLEASE INFORM THE ANESTHETIST THAT YOU HAVE A GAS BUBBLE IN THE EYE.
Q: Are there any complications?
A: As with any major surgery, there is a risk of complications. However, it is important to realise that these are generally infrequent. Complications can result in failure of the operation or loss of some or, very rarely all vision.
These include:
- Cataract (unless you have already had cataract surgery). Cataract will develop in almost all patients within 1-2 years following macular hole surgery. Surgical removal of the cataract and placement of an intraocular lens is then required.
- Retinal detachment (1-2%). This problem is usually repairable by further surgery, but visual outcomes would depend on the extent of the retinal detachment. Better outcomes are obtained if you present as soon as the symptoms of retinal detachment occur. Please see information handout on retinal detachment.
- Severe intraocular infection (less than 1:1000)
- Bleeding and total loss of vision (less than 1:1000)
Prepared by Mr. H.J. Zambarakji FRCOphth, D.M
Consultant Ophthalmic surgeon
Search the RetinaCare website
Visual guides
 Vitreomacular traction and small macular hole successfully treated with intravitreal Ocriplasmin
Vitreomacular traction and small macular hole successfully treated with intravitreal Ocriplasmin
Macular hole (pre and post op)
Epiretinal membrane (pre and post op)
Diabetic retinopathy (medical management and laser photocoagulation)
Traction diabetic retinal detachment (pre and post op)
READ HADI’S LATEST NEWS